Introduction
Dextrocardia with situs inversus, commonly known as mirror-image dextrocardia, is a rare congenital malposition of the heart where the cardiac apex is oriented to the right side. Its reported incidence is 0.01%12. Patients with dextrocardia have a normal life expectancy unless it is associated with other structural heart diseases. The incidence of atherosclerotic coronary artery disease (CAD) in these patients is presumed to be the same as that of the general population3. Owing to its rarity, there is a scarcity of data regarding coronary intervention in this subset, and the available literature is largely restricted to case reports456. Patients with dextrocardia pose a diagnostic challenge, especially in the setting of acute coronary syndrome. Clinical and electrocardiographic features and approaches to the coronary angiogram and percutaneous coronary intervention (PCI) differ. We herein describe the technical details of successful PCI in 4 cases of dextrocardia with situs inversus.
Methods
We retrospectively analysed 6 patients with dextrocardia out of 14,000 cardiac catheterisations performed in the last 15 years, from 2007-2021. These patients were evaluated for obstructive CAD and did not have any other structural heart disease. The demographic profile, procedural indications, and PCI details were analysed from the records. The continuous variables were summarised as median values. The study was in accordance with the Helsinki Convention and was approved by the institutional ethics committee for the retrospective analysis, vide No. SPL-1304, dated 24 November 2020.
Results
We had a 0.04% incidence of dextrocardia among catheterised patients evaluated for CAD. Two patients had normal epicardial coronary arteries, while 4 patients had PCI in a total of 6 coronary lesions. The median age of these 4 PCI patients was 48.5 years. Three patients presented with acute coronary syndrome, while one had chronic stable angina. The conventional risk factors of CAD of each patient are mentioned in Table 1. One patient had a normal left ventricle ejection fraction (Case 1), while the remaining 3 patients had an ejection fraction of less than 50%. The electrocardiogram (ECG) showed a negative P wave in the I and aVL limb leads, a positive R wave in the aVR limb leads, a prominent S wave in the left-sided chest leads and a prominent R wave in the right-sided chest leads (Figure 1), which is suggestive of dextrocardia with situs inversus. The ST-segment elevation in inferior limb leads (Figure 1A, Figure 1B, Case 1) and the ST-segment depression in right-sided chest leads (Figure 1C, Figure 1D, Case 2) were suggestive of inferior wall myocardial infarction and anterior wall ischaemia, respectively. Two patients had primary PCI for acute myocardial infarction, while the rest had elective/early PCI (Table 1). PCI was performed via transfemoral access for all patients. The median SYNTAX score was 16. Four lesions were of type C, while one was of type A and one of type B1. We used the conventional/routine angiographic projection technique for one patient (Figure 2), while the remaining 3 patients had a “horizontal sweep reverse” image display during PCI (Figure 3). The selective cannulations of the right coronary artery (RCA) and the left coronary artery (LCA) were performed using standard guide catheters. We performed a counterclockwise rotation of the guide catheter instead of standard clockwise rotation for the selective cannulation of the RCA. Cannulation of the LCA did not require any specific or different manoeuvre. A total of 10 stents were used in 6 lesions with a mean diameter of 3.1 mm and a mean length of 29.3 mm. The median fluoroscopy time and radiation doses were 17.9 minutes and 928 mGy, respectively. The fluoroscopic time for the first case was long (38 minutes), while the rest had shorter fluoroscopy times, despite the complex, multivessel PCI. Case 3 had sudden cardiac death at 5 months of follow-up, while the remaining 3 patients had favourable intermediate- to long-term clinical outcomes.
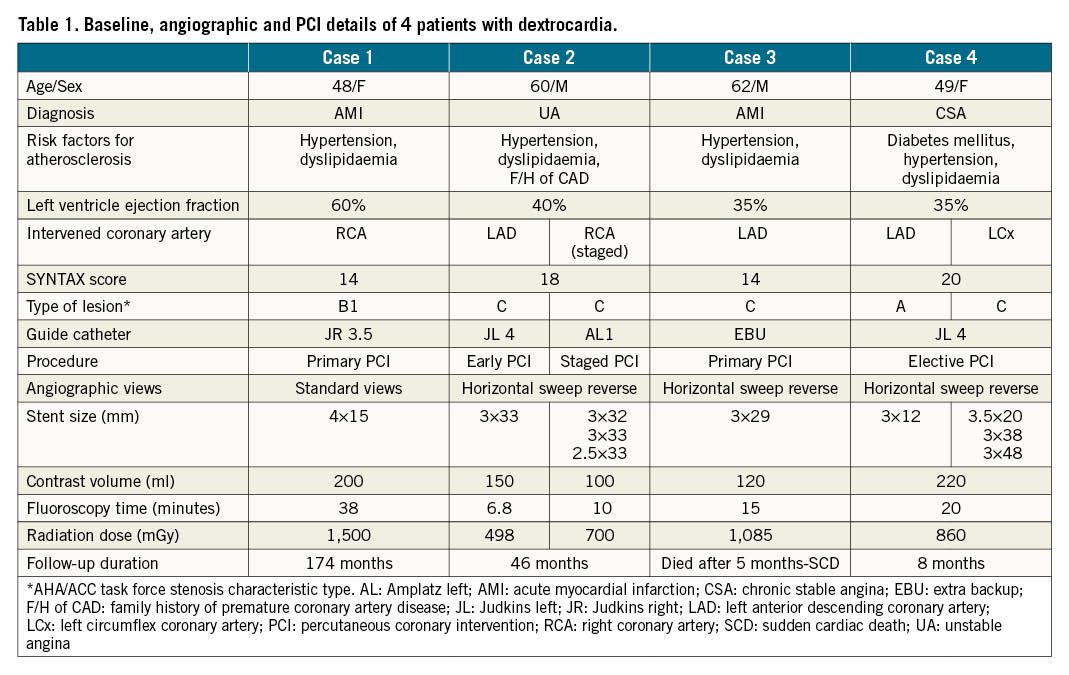
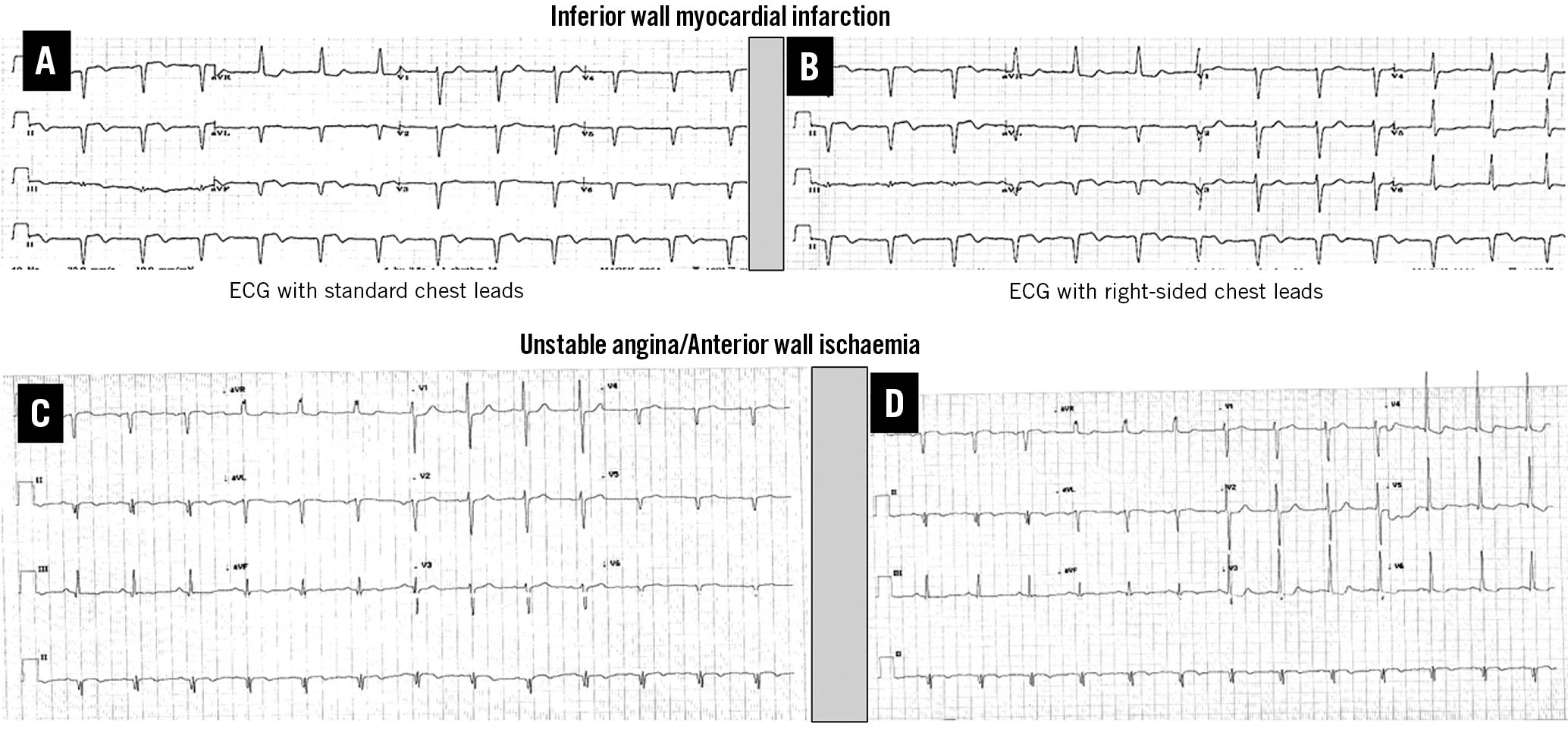
Figure 1. Electrocardiogram (ECG) with standard chest leads (A, C) and right-sided chest leads (B,D) in dextrocardia patients with situs inversus. The ECG of Case 1 (A,B) is suggestive of inferior wall myocardial infarction, while the ECG of Case 2 (C,D) is suggestive of anterior wall ischaemia.
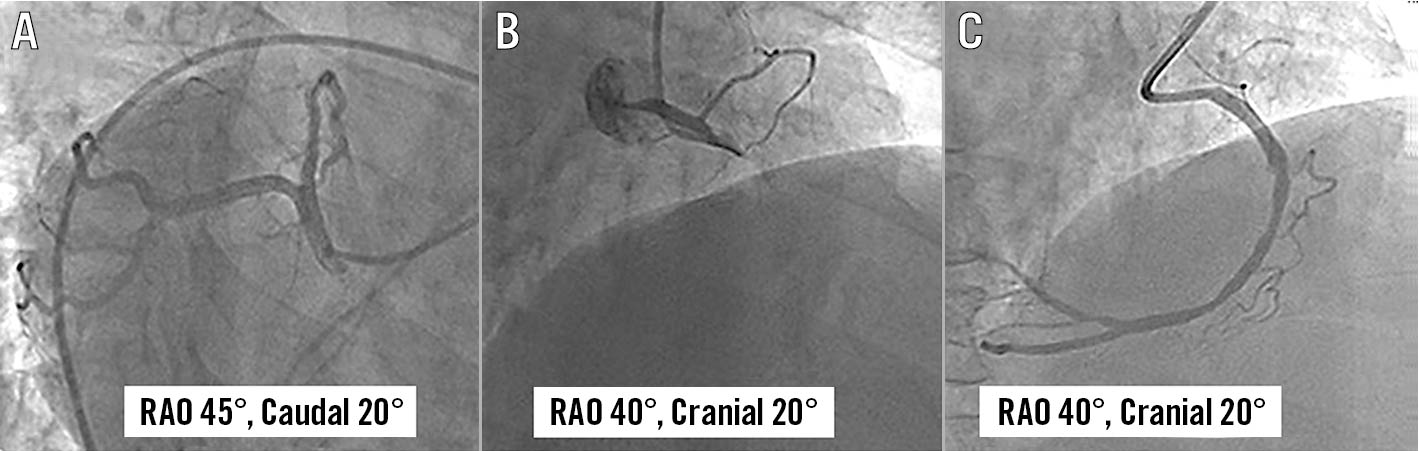
Figure 2. Coronary angiogram using the standard image display method in Case 1. Left coronary angiogram in right anterior oblique (RAO) 45°, caudal 20° (A) showed normal coronaries. Right coronary angiogram in RAO 40°, cranial 20° showed thrombotic occlusion of proximal right coronary artery (B), which was successfully stented (C).

Figure 3. Coronary angiogram using the “horizontal sweep reverse” display in Case 2. Coronary angiogram of left coronary artery in RAO 60°, caudal 20° view (A) and left anterior oblique (LAO) 30°, cranial 20° view (B) showed diffuse disease of proximal to mid-left anterior descending (LAD) artery. Coronary angiogram of the right coronary artery (RCA) in right anterior oblique (RAO) 30° view showed diffuse disease of proximal to distal RCA (C). A repeat angiogram following successful stenting of LAD in LAO 30°, cranial 20° view (D) and RCA in antero-posterior (AP) cranial 30° view (E).
Discussion
Dextrocardia with situs inversus is a rare condition with an incidence of 0.01%12. We found an incidence of 0.04% in cardiac catheterisation patients. Though the incidence of CAD is the same as that of the general population, PCI in dextrocardia is rarely encountered45678910. The published literature is on isolated case reports and their reviews45678910. The change in anatomical orientation leads to a change in the atrial and ventricular electrical axes. The classical ECG findings as described in Figure 1 and by Winter et al11 and Khalil et al12 is diagnostic of dextrocardia with situs inversus. PCI was performed through transfemoral access for all patients, though transradial access has been attempted previously by Menozzi et al 4 and Sinner et al13. The image orientation is the main concern during PCI, as suitable angiographic projection can be tricky. The standard image display in this unfamiliar anatomy may pose a technical challenge for selective cannulation of the coronary ostia during PCI. Moreyra et al14described difficulty in RCA cannulation with a Judkins catheter and instead used an Amplatz catheter. We used Judkins and Amplatz guide catheters, one in each of 2 RCA PCI cases. Instead of routine clockwise rotation of guide catheters at the aortic root, a counterclockwise rotation is recommended by Blankenship et al 15 and Ishiguro et al 16 for selective RCA cannulation. An important and useful modification of the angiographic view display through the “horizontal sweep reverse” function can make the intervention far easier610. This function, available in most catheterisation laboratories, includes reversing the right and left image displays. This leads to a more familiar and recognisable angiographic display (Figure 3), to which most interventionists are attuned. In the absence of reverse display, PCI results in higher contrast volume, fluoroscopic time and radiation dose4, as we experienced in Case 18.
Limitations
The “horizontal sweep reverse” function may not be available on all catheterisation machines. In such situations, one has to work with the standard image display, which might be technically challenging for individual operators.
Conclusions
The present case series of 4 dextrocardia with situs inversus patients highlights the importance of image reversal and catheter manipulation for selective cannulation of coronary ostia during PCI.
Conflict of interest statement
The authors have no conflicts of interest to declare.
