A 70-year-old woman with no history of cardiovascular disease was admitted to our hospital for inferior ST-segment elevation myocardial infarction. Urgent coronary angiography (CAG) revealed severe stenosis with Thrombolysis and Myocardial Infarction (TIMI) flow grade 1 in the right coronary artery (RCA) (Figure 1A, Moving image 1). Due to anterograde flow impairment and ongoing ischaemia, we dilated the lesion with a 2.0 mm balloon catheter (Sapphire II; OrbusNeich). Intravascular ultrasound (IVUS) imaging (AltaView; Terumo) clearly showed an intimal flap (Figure 1B, Moving image 2) and a massive intramural haematoma (IMH) at the proximal end of the flap. We diagnosed the patient with retrograde spontaneous coronary artery dissection (SCAD). We performed a long inflation, for 5 min, with a 2.5 mm perfusion balloon (PB) (Ryusei; Kaneka Medix) (Figure 1C). Satisfactory acute gain was achieved (Figure 1D, Moving image 3) and TIMI flow grade 3 was obtained without IMH propagation. On the 14th day of hospitalisation, CAG revealed moderate stenosis in the RCA (Figure 1E), even though the level of fractional flow reserve (FFR) was 0.95. Optical coherence tomography (OCT) and IVUS clearly showed the healed flap without IMH propagation (Figure 1F, Figure 1G, Moving image 4, Moving image 5). Therefore, we decided to defer from performing additional percutaneous coronary interventions. Three months later, the patient’s coronary computed tomography showed the lesion to be completely healed (Figure 1H, Figure 1I). Since a PB has the advantage of maintaining blood flow during balloon inflation, repeated dilatation of the target lesion for longer than several minutes was possible. Although PB have been used as bailout devices in cases of vessel perforation, occlusive dissections, and thrombotic occlusions1, long inflation using PB may be useful not only to prevent acute recoil but also to seal and heal the flap in patients with SCAD, without risk of late pathology related to metallic platforms or late malapposition due to IMH disappearance over time.
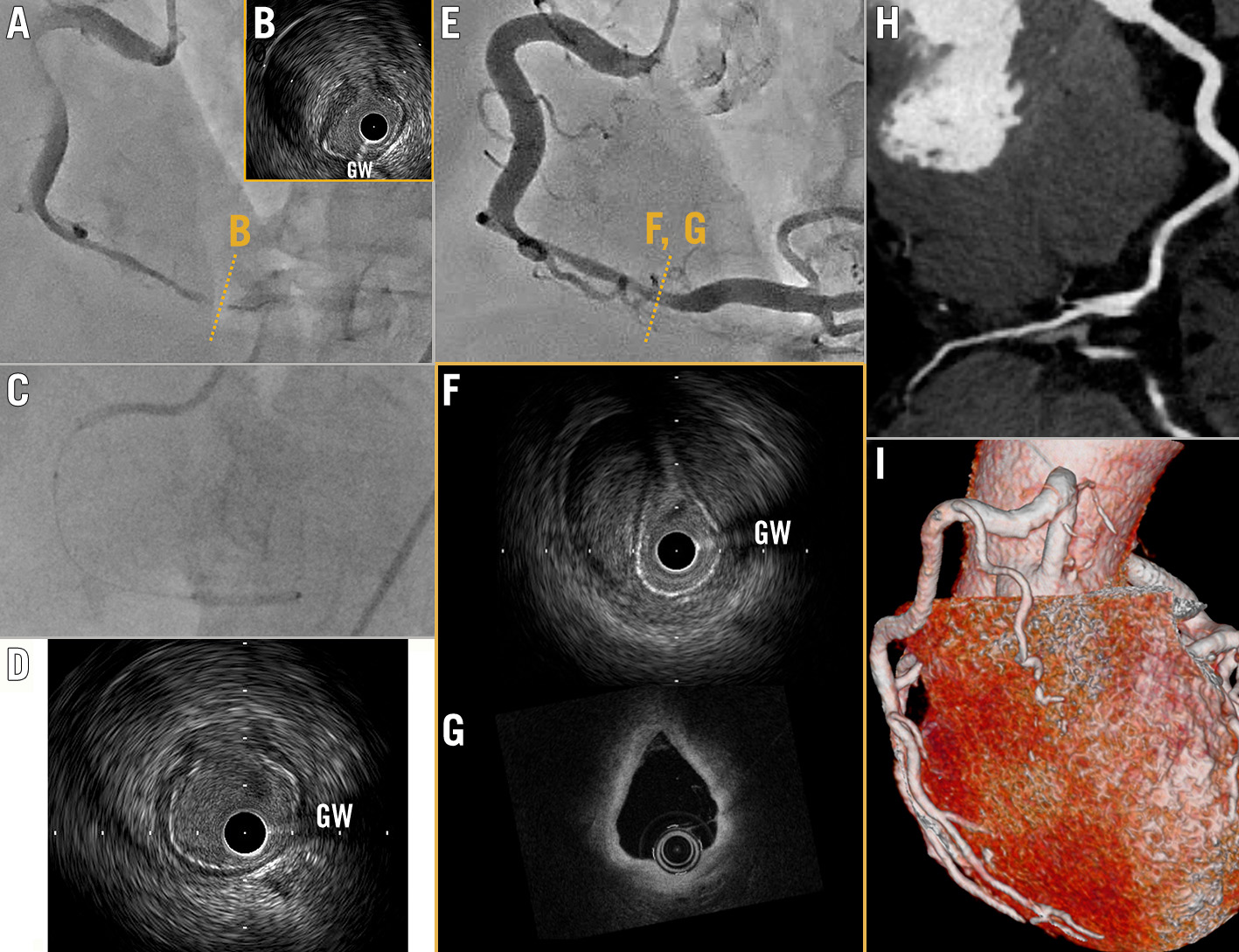
Figure 1. Intimal flap sealing with perfusion balloon. A) Coronary angiography (CAG) reveals significant stenosis in the right coronary artery. B) Intravascular ultrasound (IVUS) shows massive intramural haematoma and flap. C) Long inflation with a 2.5 mm perfusion balloon. D) IVUS shows satisfactory acute gain was achieved. E) Follow-up CAG on the 14th day of hospitalisation. F) IVUS and (G) optical coherence tomography (OCT) show the healed flap. H,I) Coronary computed tomography shows completely healed lesion 3 months later. GW: guidewire artefact
Conflict of interest statement
The authors have no conflicts of interest to declare.
