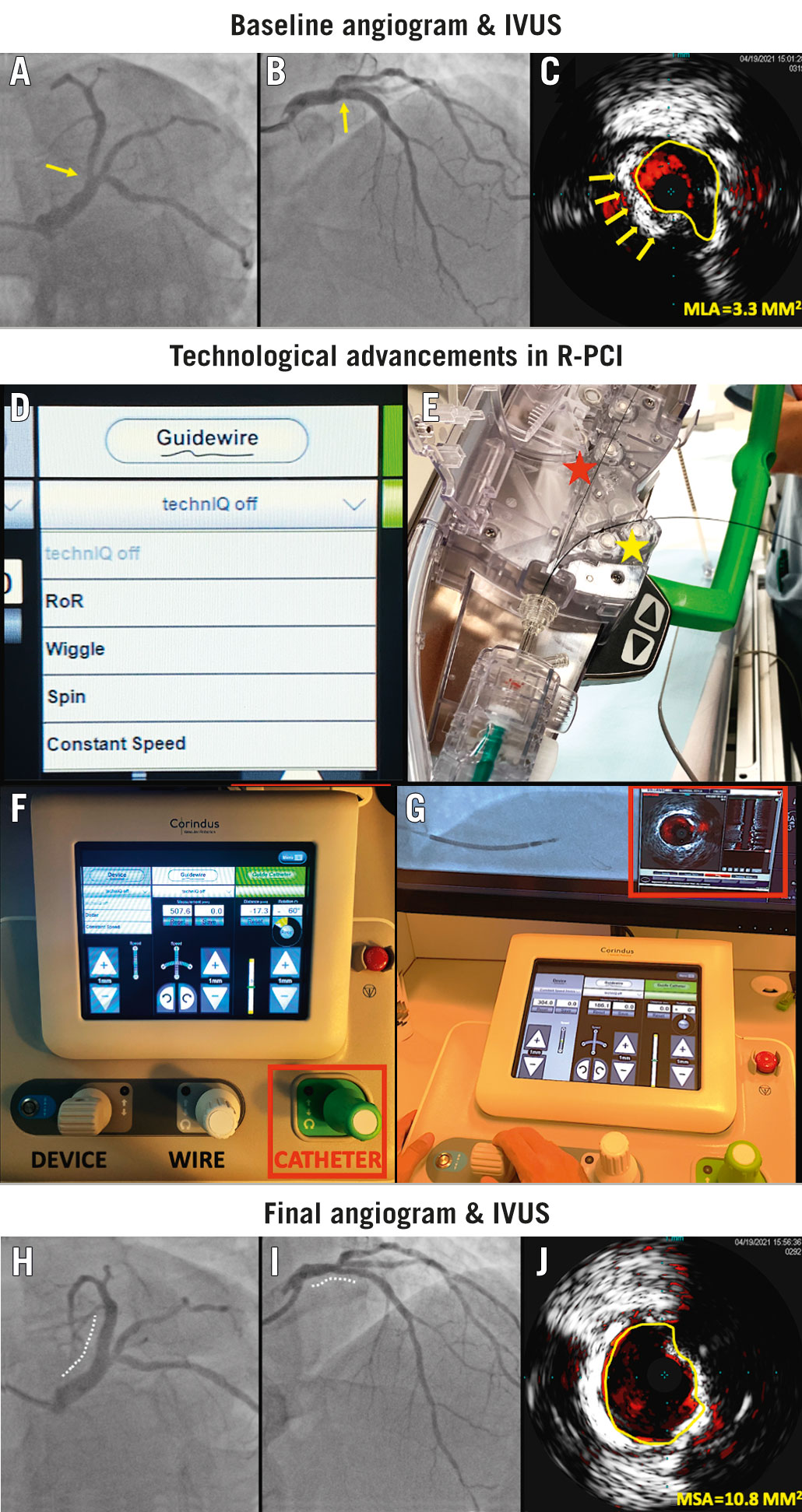
Figure 1. Robotic IVUS-guided complex PCI. A-B) Baseline angiography and (C) IVUS showing a critical calcified lesion (yellow arrow) in the ostium of the LAD, involving the left main stem and proximal LAD. D) A choice of four different automated wire controls (TechnIQ) are available to the operator. E) In addition to the “active” wire (red star), multiple additional wires and devices can be parked in the passive drive (yellow star). F) Integration of intracoronary imaging with the R-PCI system, allowing precise control of the IVUS catheter with real-time visualisation. G) The addition of guide catheter control (red box) represents a key technological development in the second-generation CorPath GRX R-PCI system. H-I) Following successful lesion predilatation, a 4.0×36 mm drug-eluting stent (Supraflex Crux) was implanted, followed by post-dilatation and proximal optimisation, yielding a good final angiographic and (J) IVUS result (Moving image 6, Moving image 7). Final procedure time was 60 minutes, fluoroscopy time 30 minutes, radiation dose 1.67 Gy and contrast volume used was 150 mls. IVUS: intravascular ultrasound; LAD: left anterior descending; R-PCI: robotic-assisted percutaneous coronary interventions
Robotic-assisted percutaneous coronary interventions (R-PCI) represent a new frontier for interventional cardiology (Supplementary Figure 1). In this image, we showcase the key technological developments in the latest-generation robotic CorPath GRX system (Corindus Vascular Robotics, Siemens Healthineers), which facilitated an intravascular ultrasound (IVUS)-guided PCI of a complex left main to the left anterior descending (LAD) artery lesion (Figure 1, Moving image 1, Moving image 2).
Lesion wiring can now be performed with the use of automated wire movements (termed TechnIQ in the CorPath GRX system), which use artificial intelligence technology to replicate common wire manoeuvres performed by operators. In this case, the critically calcified lesion was safely crossed using the “wiggle” feature, and the “spin” feature was used to advance the wire distally (Moving image 3, Moving image 4). Further automations include “rotate on retract” and “constant speed”. The ongoing NAVIGATE-GRX randomised clinical trial (ClinicalTrials.gov: NCT04883008) will compare the safety and effectiveness of using these automated wire controls. Additionally, the “dotter” and “constant speed” automations can be used to assist in the advancement of devices (balloons or stents).
Precise control of the guiding catheter is now possible, with the ability to advance, retract and rotate the guiding catheter. This allows for multiple adjustment and stabilisation manoeuvres to be performed during balloon/stent delivery and retrieval. In addition, precise control of the guiding catheter-facilitated visualisation of the entire left main stem (LMS) during IVUS pull-back. The integration of IVUS into R-PCI systems means interventionists can now optimally treat more complex lesion subtypes. However, not all IVUS catheters are compatible with the CorPath GRX system. In our case, IVUS was performed robotically using the Eagle Eye Platinum catheter (Philips) (Moving image 5).
These technological improvements in wire manipulation, guide catheter control and IVUS imaging demonstrate how R-PCI systems are evolving to overcome the challenges of contemporary PCI.
Conflict of interest statement
D. Dudek is a speaker for Siemens Healthineers. The other authors have no conficts of interest to declare.
