Yoshinobu Murasato, Nicolas Foin
AsiaIntervention 2017;3:158-159, DOI: 10.4244/AIJ-D-16-00020
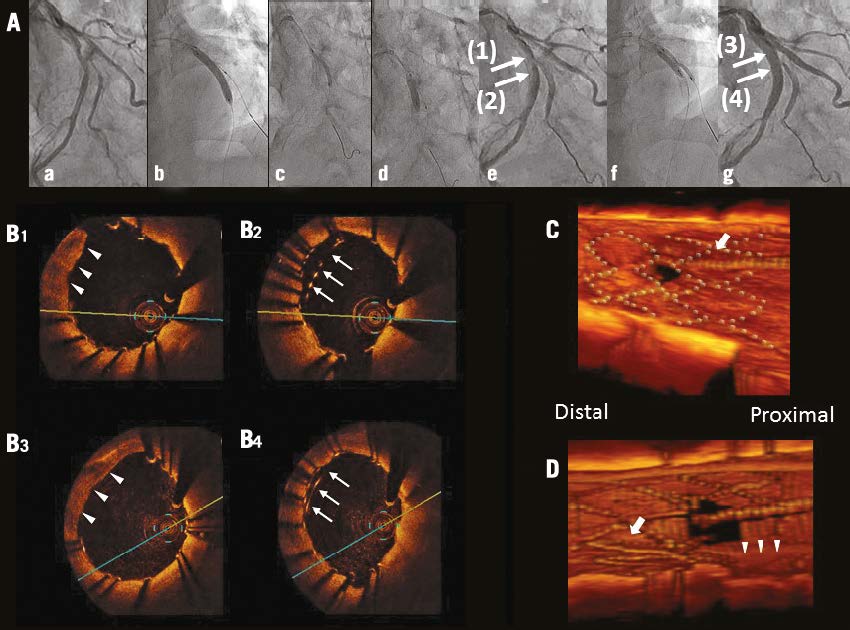
A 64-year-old male underwent percutaneous coronary intervention (PCI) for a 1,1,1 lesion in the left anterior descending artery (LAD)-diagonal (Dx) bifurcation (Panel Aa). A biolimus-eluting 3.5/24 mm stent (Nobori®; Terumo Corp., Tokyo, Japan) was implanted in the middle LAD (Panel Ab) followed by respective sequential dilations of Dx and LAD with 2.0 mm (Panel Ac) and 3.5 mm balloons (Maverick²™; Boston Scientific Corp., Marlborough, MA, USA, and Raiden 3; Kaneka Medix, Osaka, Japan, respectively) (Panel Ad) after guidewire (GW) recrossing (Panel Ae). Finally, a kissing balloon inflation (KBI) was then performed (Panel Af, Panel Ag), after optical coherence tomography (OCT) showed an unscaffolded area proximally (Panel B1) and double layered struts distally to the bifurcation (Panel B2). Although the strut-unscaffolded area remained proximally (Panel B3), KBI improved the malapposition of the distal double strut layer (Panel B4).
The three-dimensional OCT images reconstructed after the intervention clearly showed the GW recrossing through a proximal cell into the Dx ostium (Panel C, arrow). The jailed struts were then deflected distally after respective Dx and LAD dilations (Moving image 1). These struts protruding in the lumen distal to the Cx were subsequently reapposed after KBI (Panel D, arrows) but an area uncovered by stent struts remained proximally (triangles). GW recrossing in the optimal distal cell leads to adequate side branch dilation and less incomplete stent apposition. GW recrossing in the proximal cell has been reported to cause protrusion of the jailed struts into the main vessel, and the present case suggests a potential risk of struts protruding distally into the main vessel after proximal rewiring. Malapposed struts in the bifurcation and incomplete apposition of the double-layered struts in complex stenting have been reported to increase the risk of stent thrombosis and restenosis. Three-dimensional OCT was useful to identify accurately GW recrossing and the cause of strut deformation and malapposition.
Moving image 1. Final three-dimensional OCT.
To download the full article, please click below.