Umihiko Kaneko, Yoshifumi Kashima, et al
AsiaIntervention 2017;3:164-165, DOI: 10.4244/AIJ-D-16-00031
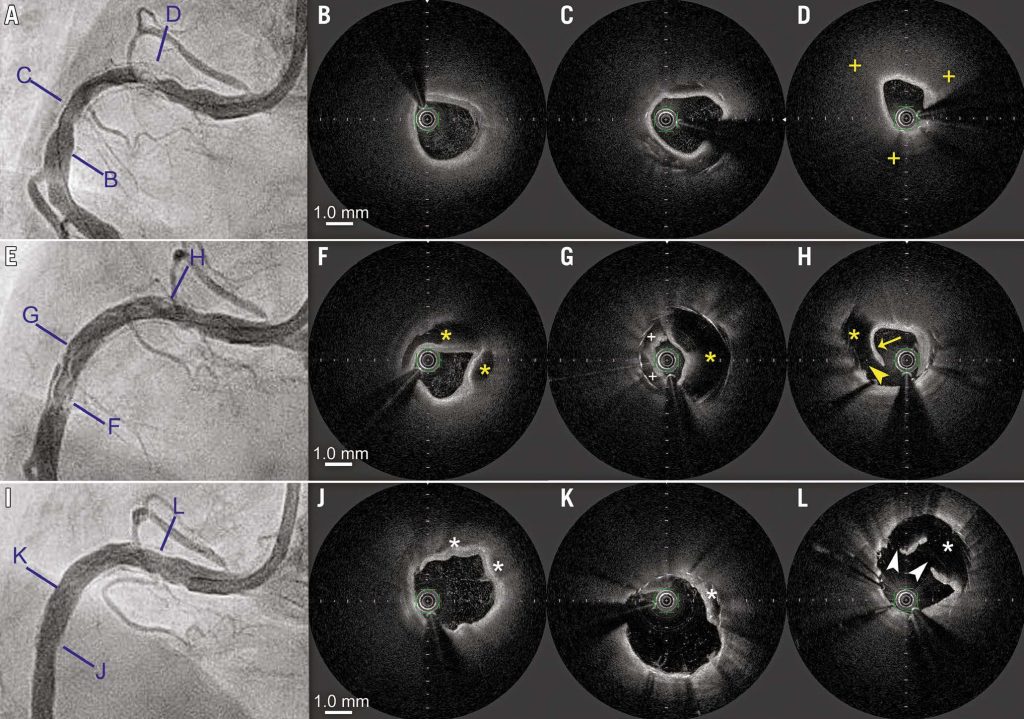
A 75-year-old woman who was implanted with a 3.0×28 mm biolimus-eluting stent in the proximal right coronary artery two years previously presented with unstable angina due to focal in-stent restenosis (Panel A). Optical frequency domain imaging (OFDI) (Terumo Corp., Tokyo, Japan) revealed a normal pattern of homogeneous neointimal hyperplasia (Panel B, Panel C) and neoatherosclerosis with a lipid-laden neointima and large lipid pool at the most stenotic lesion (Panel D, Moving image 1). After excimer laser coronary angioplasty (1.4 mm concentric) with concomitant saline flushing, angiography revealed sudden extended multilayered haziness (Panel E, Moving image 2). OFDI clearly demonstrated extensive neointimal dissection (Panel F-Panel H, yellow asterisks, Moving image 3), some mural thrombus (Panel G, plus signs), disruption of the neointima (Panel H, arrowhead), and a mobile flap at the lasing site (Panel H, arrow), confirming neoatherosclerosis rupture complicated by extensive neointimal dissection. After angioplasty with a 3.5×13 mm scoring balloon at 20 atm and a 3.5×30 mm paclitaxel-coated balloon at 12 atm, reentry between the true lumen and dissected lumen was successfully obtained (Panel I, Moving image 4). OFDI revealed remarkable decompression of the dissected lumen (Panel J-Panel L, asterisks, Moving image 5) and several incisions (Panel L, arrowheads) created by scoring balloon angioplasty.
In-stent neoatherosclerosis has emerged as an important mechanism of drug-eluting stent failure, including delayed restenosis and very late stent thrombosis. To the best of our knowledge, this is the first report of OFDI for intraprocedural rupture of neoatherosclerosis causing extensive neointimal dissection. Although the process of this phenomenon remains unclear, the present case raises two important clinical issues: (1) some interventional procedures for neoatherosclerosis with a lipid-laden neointima and large lipid pool might carry a risk of neoatherosclerosis rupture, which can lead to extensive neointimal dissection; and (2) OFDI was crucial to elucidate the underlying mechanism and manage it successfully.
Moving image 1. Baseline OFDI, showing development of in-stent neoatherosclerosis with a lipid-laden neointima and large lipid pool.
Moving image 2. Angiography after treatment with excimer laser coronary angioplasty, showing sudden development of multilayered haziness.
Moving image 3. OFDI after treatment with excimer laser coronary angioplasty, showing ruptured neoatherosclerosis complicated with extensive neointimal dissection, disrupted neointima, and mobile flap at the lasing site.
Moving image 4. Post-procedural coronary angiography, showing restored good coronary flow and improvement of neointimal dissection.
Moving image 5. Post-procedural OFDI, showing the incision on the dissected neointima, remarkable decompression of the dissected lumen, and successful fenestration between the true lumen and dissected lumen.
To download, please click below.