Significant tricuspid regurgitation (TR) portends a poor prognosis irrespective of aetiology1. The Cardiovalve system (Venus Medtech) is a novel transcatheter replacement therapy for both mitral and tricuspid valves (TV). The Cardiovalve transcatheter tricuspid valve replacement (TTVR) system is delivered through a 32 Fr sheath and consists of a trileaflet scallop-shaped bovine pericardial valve, connected to a self-expanding nitinol frame, a covered flange at the atrial side for sealing off paravalvular leak (PVL), and 12 grasping legs for secure subvalvular anchoring. It is currently available in three sizes, covering the intracommissural annulus from 36 mm to 53 mm. Herein, we report the first compassionate-use experience with the Cardiovalve TTVR in the Asian population.
Our patient is a 60-year-old male suffering from recurrent heart failure symptoms (New York Heart Association Class III) and ascites requiring regular drainage, secondary to torrential atrial functional TR (effective regurgitant orifice area 1.35 cm2). His transoesophageal echocardiogram (TOE) showed a wide coaptation gap (11.8 mm) rendering transcatheter edge-to-edge repair (TEER) infeasible (Supplementary Figure 1, Moving image 1). He also had mild precapillary pulmonary hypertension that was responsive to macitentan (change in mean pulmonary pressure from 24 mmHg to 23 mmHg, in pulmonary capillary wedge pressure from 12 mmHg to 15 mmHg, and in pulmonary vascular resistance from 4.29 Wood units [WU] to 2.7 WU), and moderate right ventricular (RV) dysfunction (three-dimensional RV ejection fraction 43%, tricuspid annular plane systolic excursion 16 mm). His TRI-SCORE for open TV surgery was 22% thus the Heart Team recommended TTVR. Compassionate use of the Cardiovalve device was then approved by the Hong Kong regulatory board.
Cardiovalve TTVR was performed under general anaesthesia with TOE guidance. Following right femoral venous access, a 24 Fr sheath was inserted. A medium curl Agilis steerable catheter (Abbott) was positioned at the right atrium to pass a 6 Fr pigtail catheter through to the right ventricular apex and then exchanged for a Safari XS guidewire (Boston Scientific). Afterwards, a 30 mm Coda Balloon Catheter (Cook Medical) was gently moved back and forth from the right atrium to the RV to ensure the guidewire trajectory was free of chordae entrapment (Supplementary Figure 2, Moving image 2). The 32 Fr Cardiovalve XL device was then inserted over the Safari wire. The atrial capsule was steered to the best coaxial and concentric position to the TV under TOE guidance whilst keeping the distal edge of the atrial capsule above the native valve leaflets (Supplementary Figure 3, Moving image 3). Then the atrial capsule was retracted to expose the grasping legs by rotating the atrial capsule knob clockwise (Figure 1A–Figure 1B, Moving image 4). The system was then advanced across the TV and retracted to engage the leaflets. After confirming all ventricular legs were beneath the leaflets and engaged with the annulus at the same level under three-dimensional TOE multiplanar reconstruction, the atrial flange and ventricular portion of the Cardiovalve were sequentially deployed (Figure 1C–Figure 1D–Figure 1E, Moving image 5). Follow-up TOE the next day showed trivial PVL only, with slightly worsened right ventricular function (RV ejection fraction 39%, trace tricuspid regurgitation with a mean gradient 2-3 mmHg).
Tricuspid TEER has demonstrated the ability to improve quality of life in patients with severe symptomatic TR2. However, not all anatomies are feasible for TEER, whereas TTVR offers complete or near-complete elimination of TR. Currently, whether transcatheter repair or replacement should be the primary intervention modality for TR remains unclear. Nonetheless, Asian patients tend to present at an advanced stage and an unfavourable anatomy for TEER is not uncommonly seen. The early introduction of different TTVR devices to Asia would therefore potentially expand interventional options in this population.
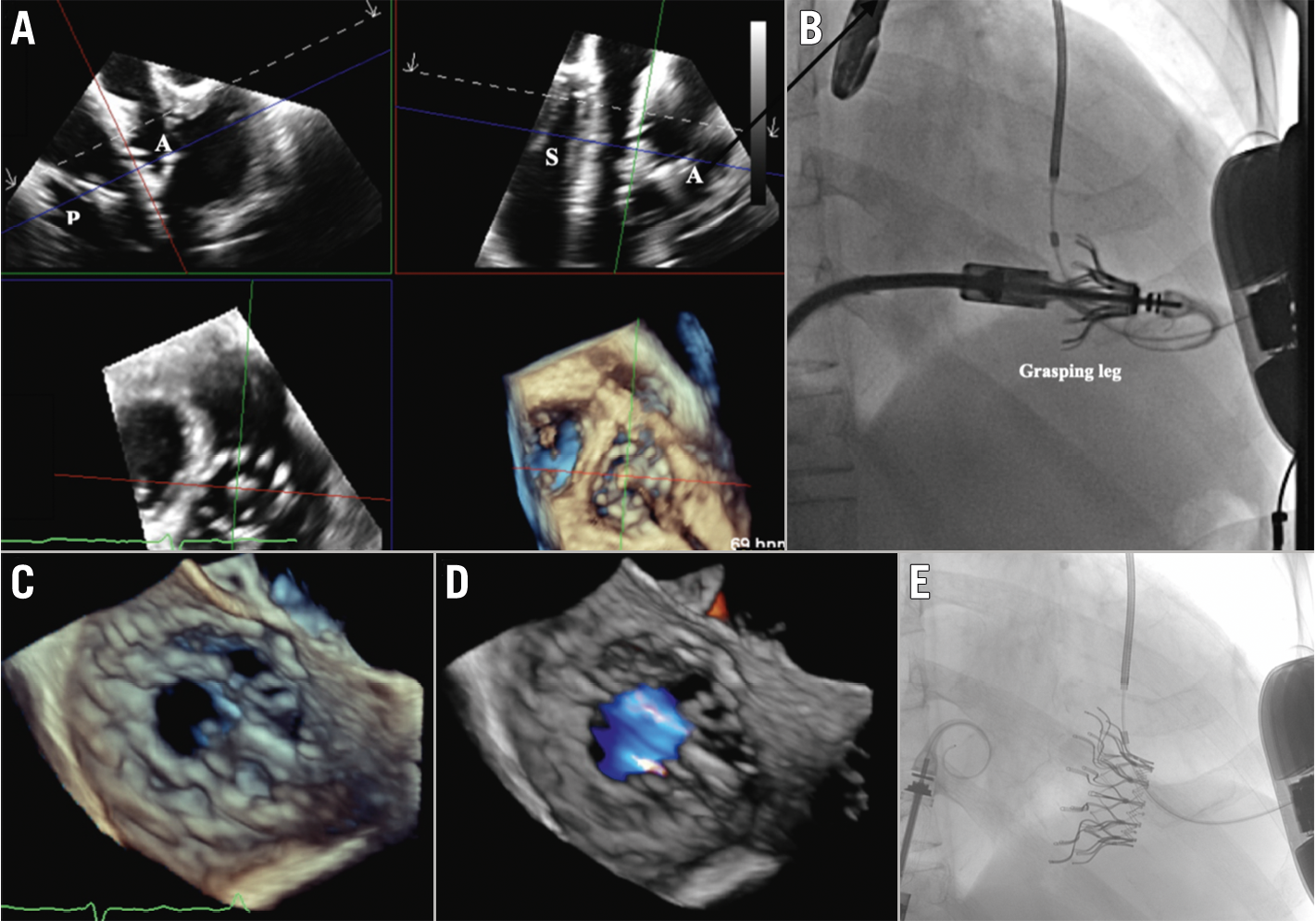
Figure 1. Cardiovalve implantation for tricuspid valve regurgitation. A) Multiplanar transoesophageal echocardiograms showing the 12 grasping legs (GL) exposed by retracting the atrial capsule. B) The exposed GL of Cardiovalve TTVR under fluoroscopy. Successful deployment of Cardiovalve TTVR under transoesophageal echocardiography (C & D) and fluoroscopic guidance (E). A: anterior; P: posterior; S: septal; TTVR: transcatheter tricuspid valve replacement
Conflict of interest statement
K. Chak-yu So is a clinical proctor for Abbott, Boston Scientific, Edwards Lifesciences, and Medtronic. The other authors have no conflicts of interest to declare.
