A 62-year-old female presented with non-ST-segment elevation myocardial infarction with right ventricular (RV) failure. An electrocardiogram showed T-wave inversion over the inferior leads. High-sensitivity troponin I was raised from normal to 17,890 ng/L (reference value <15.6 ng/L). The patient was hypotensive and dependent on inotropes. Echocardiography revealed a normal left ventricular ejection fraction but a dilated RV with impaired systolic function. Urgent computed tomography showed no aortic dissection or pulmonary embolism.
Coronary angiography showed spiral dissection arising from the ostial right coronary artery (RCA) with complete obstruction (Figure 1A). In view of haemodynamic compromise, percutaneous coronary intervention (PCI) was attempted. A Runthrough NS guidewire (Terumo) was passed into the distal RCA, but intravascular ultrasound (IVUS) showed that it was in the false lumen (Figure 1B). There was spontaneous coronary artery dissection (SCAD) arising from the ostial RCA with significant compression on the true lumen. Under real-time IVUS (AltaView [Terumo]) guidance, another Runthrough NS guidewire was passed into the true lumen successfully (Figure 1C, Figure 1D, Moving image 1). Cutting balloon angioplasty was performed (WOLVERINE [Boston Scientific]) to create fenestration between the true and false plane in order to re-establish coronary flow (Figure 1E). Drug-eluting stents were deployed from the ostial to distal RCA under IVUS guidance, covering the entire dissection segment (Figure 1F). The patient was able to wean off inotropic support and was discharged on post-op day 5.
IVUS is the imaging modality of choice to diagnose SCAD. PCI is indicated in case of no-flow or when complications were arising from SCAD, such as haemodynamic compromise, as in this case. PCI is often difficult, as the true lumen is usually compressed. Hereby, we have described the use of real-time IVUS-guided wiring of the true lumen in SCAD. Since further injection of contrast should be avoided to prevent extension of the dissection, the use of IVUS for accurate ostial stent placement should also be considered1.
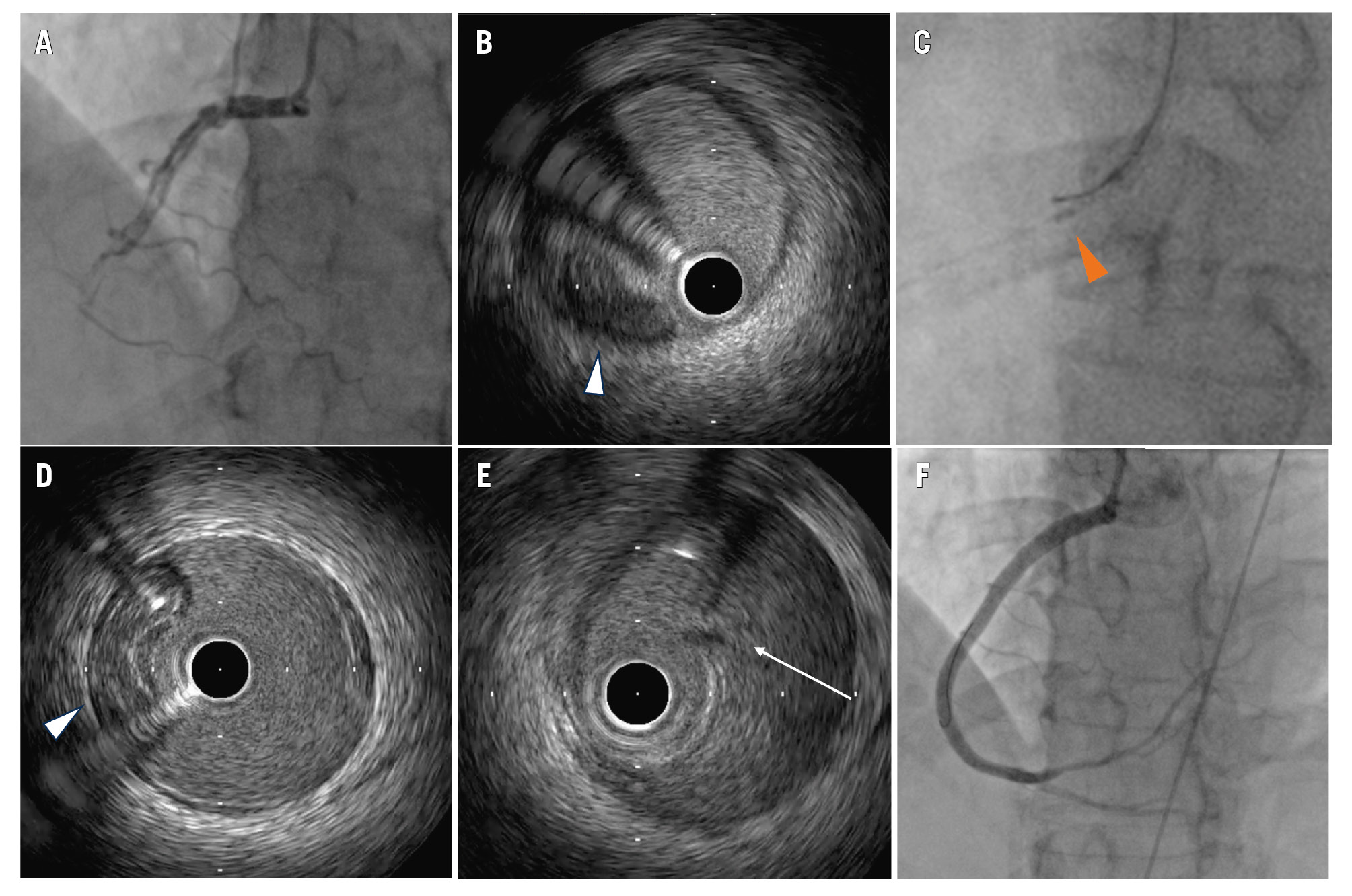
Figure 1. IVUS-guided wiring in a patient with SCAD. A) Baseline angiogram showing ostial RCA SCAD. B) IVUS image of SCAD showing a compressed true lumen (white arrowhead). C) Fluoroscopic image of real-time IVUS-guided wiring (orange arrowhead: IVUS probe). D) IVUS confirmed true luminal wiring (white arrowhead). E) IVUS image after cutting balloon angioplasty showing fenestration of the dissection flap (white arrow). F) Final angiographic result. IVUS: intravascular ultrasound; RCA: right coronary artery; SCAD: spontaneous coronary artery dissection
Guest Editor
This paper was guest edited by Davide Capodanno, MD, PhD; A.O.U. Policlinico “G. Rodolico-San Marco”, University of Catania, Catania, Italy.
Conflict of interest statement
The authors have no conflicts of interest relevant to the contents of this paper to declare. The Guest Editor has no conflicts of interest to declare relevant to the contents of this paper.
