A 66-year-old man underwent transcatheter mitral valve repair for severe functional mitral regurgitation (MR) due to dilative cardiomyopathy.
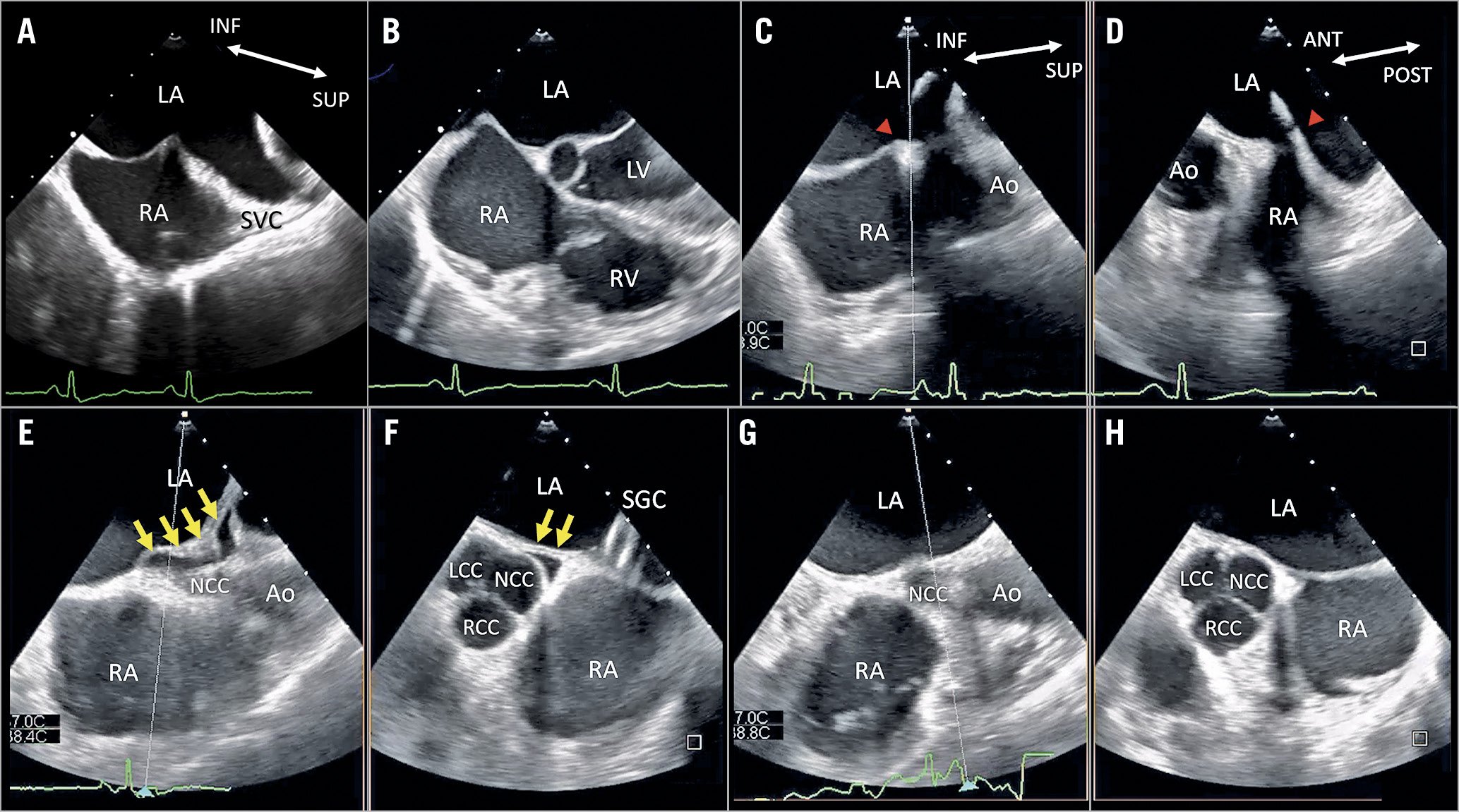
There was no pericardial effusion (PE) (Panel A, Panel B, Moving image 1, Moving image 2), and transseptal puncture (TSP) was performed in the superior and anterior fossa ovalis without complications. Transoesophageal echocardiography (TEE) (EPIQ7/X8-2t system; Philips, Andover, MA, USA) revealed that the steerable guide catheter (SGC) was pulling the osseous membrane and causing it to tent as it was inserted into the left atrial (LA) cavity (Panel C, Panel D, Moving image 3). A MitraClip G4 NTW® (Abbott Vascular, Santa Clara, CA, USA) was successfully implanted once the MR had reduced. When the clip delivery system was removed from the SGC, TEE revealed a pericardial space between the LA wall and aortic root, indicating PE) (Panel E, Panel F, Moving image 4). No PE was observed elsewhere, and the vital signs remained unchanged, thereby excluding cardiac tamponade. The procedure was immediately terminated. However, the PE disappeared once the SGC was removed and did not return (Panel G, Panel H, Moving image 5, Moving image 6).
PE between the LA wall and aortic root is common. This fatal complication of TSP stems from improper puncture of the fossa ovalis1. However, we detected no such punctures using TEE. There is a pericardial sac, which has a double-walled structure, surrounded by the LA, right atrium, and base of the aortic root. We suspected that the redundant LA wall and pericardium were pulled due to excess tension generated by the SGC and displaced in the direction of the LA cavity, thereby creating free space. The Heart Team should consider pseudo-PE when excess tension is generated by the SGC during the MitraClip procedure.
Conflict of interest statement
The authors have no conflicts of interest to declare.
