With great interest, I read the paper by Shao-Liang Chen published in your Journal entitled “DEFINITION criteria for left main bifurcation stenting − from clinical need to a formula”1. The author correctly mentions the major limitations of the Medina bifurcation classification: “However, this classification also has limitations because it doesn’t include important descriptive features of bifurcation lesions that could be helpful in determining the optimum stent treatment strategy. Therefore, the lack of a comprehensive stratification system defining the complexity of bifurcation lesions remains an unmet clinical need”. Another detailed classification system, called the Movahed bifurcation classification system, exists that is simpler than the Medina classification in its basic structure and has unlimited suffixes that can be added in order to describe any given bifurcation lesion anatomy for clinical or research purposes. The Movahed classification23 simplifies bifurcation lesions into three categories: in the so-called B2 (B for bifurcation, 2 for both branches), both branches are involved; if only the main branch is involved, it is called B1m (B for bifurcation, 1m meaning only the main branch has disease); and if only the side branch is involved, it is called a B1s lesion (B for bifurcation and 1s meaning only the side branch has the disease). Next, the Movahed classification adds additional optional suffixes that can describe any anatomical features of a given bifurcation classification that are needed for specific clinical or research purposes, enabling succinct definitions. For example, describing the angiographic criterion that was used in the DEFINITION study was a lengthy affair, whereas, using the Movahed bifurcation classification, it could have been summarised as follows: B2LM SBL ≥10 mm SBSD ≥70% CA MVD <2.5 TR MVL ≥25 (B2: both branches have the disease; LM: left main lesion; SBL ≥10 mm: side branch lesion length over 10 mm; SBSD ≥70%: side branch stenosis diameter ≥70%; CA: significant calcification; MVD <2.5: main vessel diameter <2.5 mm; TR: thrombus-containing; MVL ≥25: main vessel lesion length ≥25 mm). We believe the widely used Medina bifurcation classification should be abandoned in favour of the Movahed classification due to the complexity and lack of suffixes, in the former, for describing any needed anatomical description of a given coronary bifurcation lesion45678. Figure 1 and Figure 2 describe the Movahed classification in comparison to the Medina classification with a detailed description of the Movahed classification when using additional suffixes.
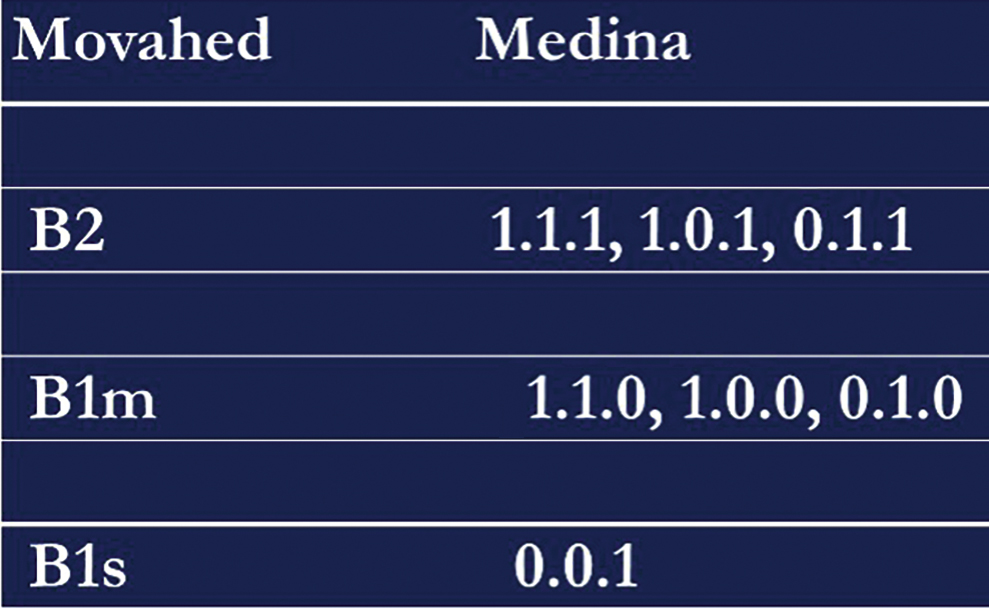
Figure 1. Comparison of the Movahed to the Medina coronary bifurcation classification revealing the simplicity of the basic suffix of the Movahed classification.
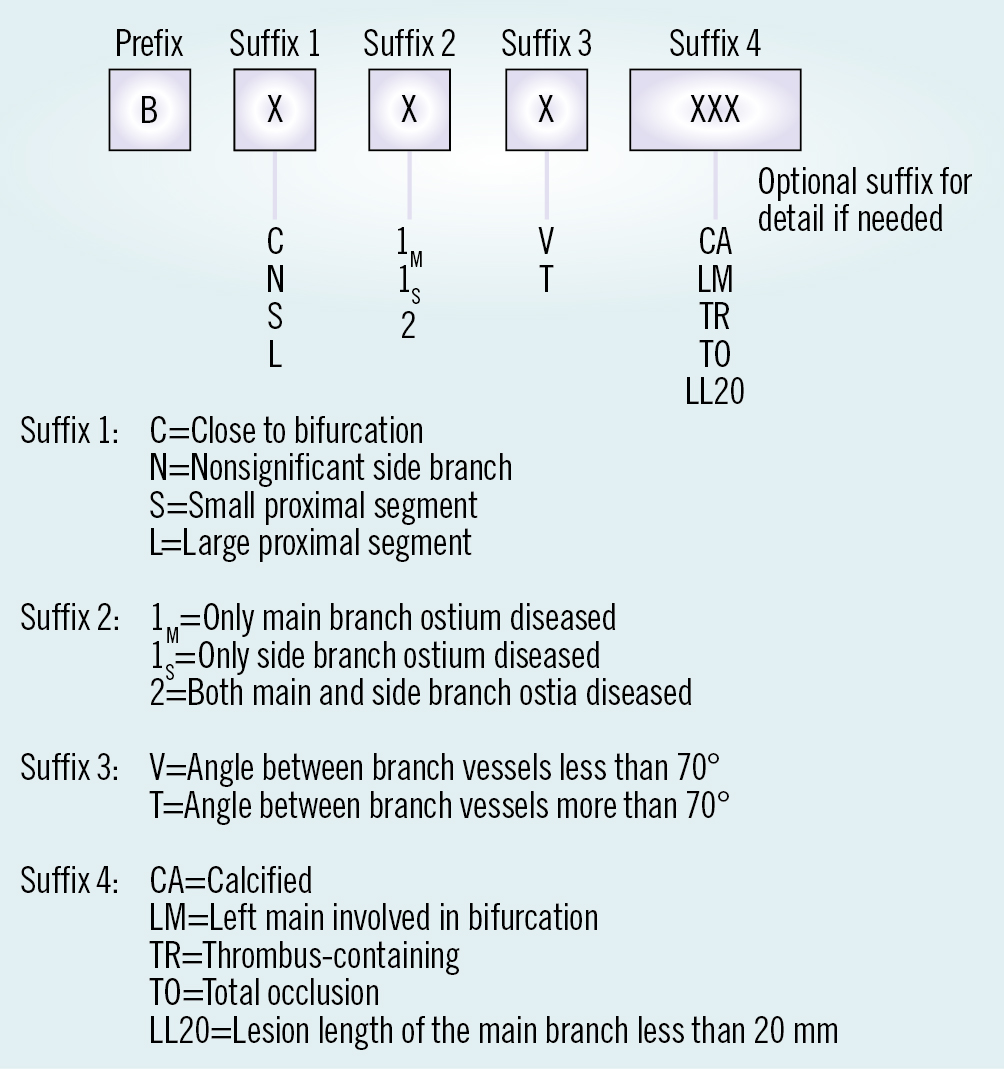
Figure 2. Details of the Movahed bifurcation classification with limitless optional suffixes.
Conflict of interest statement
The author has no conflicts of interest to declare.
