Provisional stenting remains the predominant strategy for managing most coronary bifurcation lesions1. However, a key limitation of this approach is the risk of side branch (SB) compromise or occlusion following main vessel (MV) stenting. Jailed-balloon techniques (JBTs), previously described in the literature, provide a safe and effective method of SB protection during MV provisional stenting, particularly in lesions deemed at high risk of SB compromise2. Nevertheless, certain iterations of these techniques may be associated with balloon-induced vascular injury, especially in the presence of ostial or proximal SB disease, potentially leading to increased rates of restenosis and target lesion revascularisation.
Drug-coated balloons (DCBs) deliver antiproliferative agents that promote endothelial healing and inhibit neointimal hyperplasia3, and these can be used in place of standard balloons in the SB during complex, non-left main bifurcation interventions. Here, we describe a variation of the JBT that incorporates a DCB in the SB – termed the jailed DCB technique (JDT) – for provisional stenting of a left anterior descending artery (LAD) and diagonal bifurcation (Figure 1). Following intravascular ultrasound (IVUS) assessment, both the MV and the SB were prepared using compliant and scoring balloons. Through a 6 Fr Vista Brite Tip XB 3.0 guiding catheter (Cordis), a 3.5×28 mm XIENCE Sierra drug-eluting stent (Abbott) and a 2.5×20 mm Prevail DCB (Medtronic) were positioned in the MV and SB, respectively. The proximal marker of the jailed DCB, which was size-matched angiographically to the SB diameter, was positioned within the MV stent. The DCB was inflated first, followed by the stent, both to nominal pressures. The stent balloon was then deflated while the DCB was left inflated for 60 seconds, allowing full transfer of the drug, before deflation and removal of both used balloons. Proximal optimisation technique and distal stent optimisation were subsequently performed. The final angiogram demonstrated widely patent LAD and diagonal branches, with a well-optimised MV stent confirmed by IVUS imaging. The patient remained clinically well at the follow-up visits at 6 weeks and 6 months.
Bench testing of the JDT was also performed using silicone models of coronary bifurcation (Terumo) (Supplementary Figure 1). No evidence of major MV stent distortion or vessel wall malapposition was seen. Notably, the difficulty experienced during jailed balloon removal was comparable to the one felt when removing a jailed wire.
The JDT represents a promising advancement of the jailed-balloon strategy for bifurcation percutaneous coronary intervention. By integrating effective SB protection with localised antiproliferative drug delivery, this approach may reduce the risk of SB compromise and balloon-induced vascular injury seen with conventional methods. In the presented case and supporting bench testing, the JDT demonstrated technical feasibility, procedural safety, and favourable short-term outcomes without evidence of stent distortion or malapposition. Further clinical studies are needed to confirm these findings and establish the long-term safety and efficacy of this technique in complex, non-left main bifurcations.
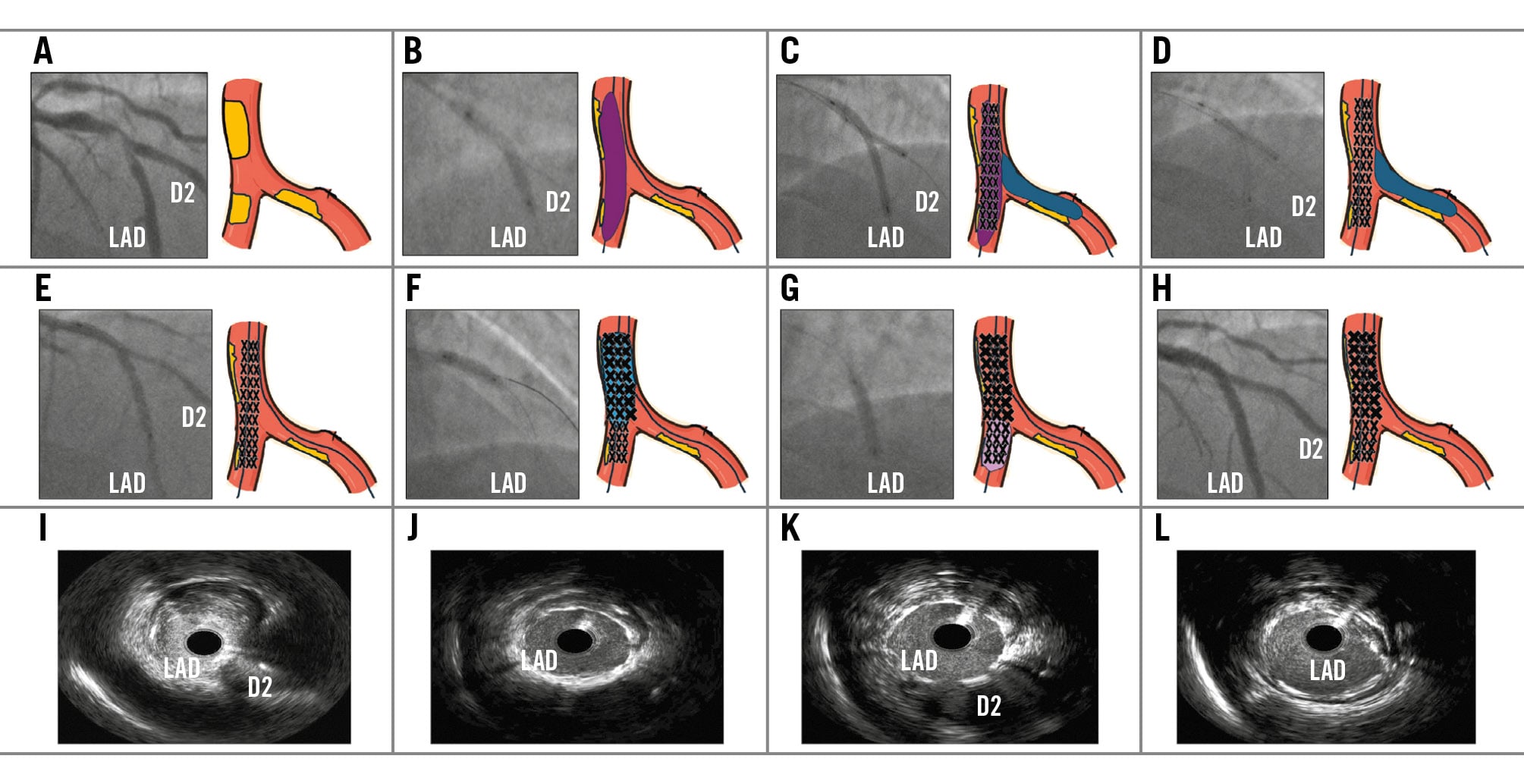
Figure 1. Actual case, simulation, and IVUS images of the jailed drug-coated balloon technique. A) Angiogram and cartoon simulation of complex left anterior descending artery (LAD) and diagonal 2 (D2) bifurcation; (B) wiring and predilation of the LAD; (C) Prevail drug-coated balloon (DCB; Medtronic) in D2 inflated first, followed by inflation of the XIENCE Sierra stent (Abbott) in the LAD; (D) deflation of the stent balloon while the DCB in D2 is left inflated for 60 seconds; (E) result after deflation and removal of both balloons; (F) proximal optimisation of the LAD stent; (G) optimisation of the LAD stent; (H) final result; (I) intravascular ultrasound (IVUS) image preintervention at the LAD/D2 bifurcation; (J) IVUS image post-intervention just distal to the bifurcation; (K) IVUS image post-intervention at the LAD/D2 bifurcation; (L) IVUS image post-intervention just proximal to the bifurcation.
Patient consent statement
Written informed consent was given by the patient for his information to appear in a journal article destined for publication.
Acknowledgements
Written informed consent was given by the patient for his information to appear in a journal article destined for publication.
Conflict of interest statement
The authors have no conflicts of interest to declare.
