An 82-year-old male presented with exertional angina. Coronary angiography showed a severe mid-left anterior descending artery (LAD) and second diagonal (D2) bifurcation lesion (Medina 1,1,1) (Figure 1A). Baseline optical coherence tomography (OCT) pullbacks were performed in the LAD and D2 arteries, followed by predilatation with a 2.75 mm non-compliant (NC) balloon in both branches and a 3.0×10 mm cutting balloon in the LAD. A 2.75×12 mm XIENCE Skypoint (Abbott) drug-eluting stent (DES) was deployed in the D2, with minimal protrusion into the LAD (Figure 1B). Following post-dilatation with a 3.0×12 mm NC balloon, a new guidewire was looped into the D2 and carefully pulled back to rewire the LAD through the minimally protruding stent strut. OCT pullback was performed from the D2, and the three-dimensional (3D) bifurcation view confirmed the guidewire position through the first protruding strut (Figure 1C, Moving image 1). The first kissing balloon inflation (KBI) was performed with two 3.0×12 mm NC balloons (Figure 1D), and a 2.75×28 mm XIENCE Skypoint DES was deployed in the LAD (Figure 1E). Proximal optimisation technique (POT) was performed with a 3.5×8 mm NC balloon (Figure 1F). The D2 was then rewired through the distal cell, which was confirmed with OCT pullback from the LAD (Figure 1G, Moving image 2). A second KBI was then performed (Figure 1H), followed by coverage of a proximal edge dissection with a 3.0×8 mm DES and final POT (Figure 1I, Figure 1J). The final OCT pullback showed good stent results, including a widely open D2 ostium without excess metal at the carina (Figure 1K, Moving image 3). The final angiographic result is shown in Figure 1L.
OCT-guided percutaneous coronary intervention (PCI) in complex bifurcation lesions has been shown to reduce major adverse cardiovascular events in the Optical Coherence Tomography Optimized Bifurcation Event Reduction (OCTOBER) Trial1. Optimising stent outcomes for OCT-guided double-kissing (DK) crush or culotte can be demanding, requiring a minimum of six OCT pullbacks per case (pre- and post- for both branches, and once after each rewiring). This may limit its use in patients with renal impairment, unless a saline flush is used for OCT assessment. Proximal versus distal stent cell rewiring is important depending on the type of bifurcation strategy used and can be confirmed by 3D-enhanced OCT. The DK single-string culotte is an attractive variation of culotte stenting that minimises stent overlap in the main vessel while ensuring coverage of the side branch ostium234. This technique is appropriate in bifurcation anatomies such as those described for other forms of culotte, i.e., similar main vessel and side branch sizes and a bifurcation angle <70°. Beyond anatomical considerations, operator experience in the chosen two-stent bifurcation technique is equally important to achieve optimal outcomes5.
The main challenge of the DK single-string culotte lies in the precise amount of protrusion of the side branch stent. If more than one strut is protruding into the main vessel, the distal cell should be rewired before balloon dilatation to avoid an excessive metallic neocarina, converting the case into a mini-DK culotte. One strut protrusion to perform DK single-string culotte is usually only demonstrable by 3D-OCT, as in this case example. Insufficient protrusion will likely convert the case into T-stenting.
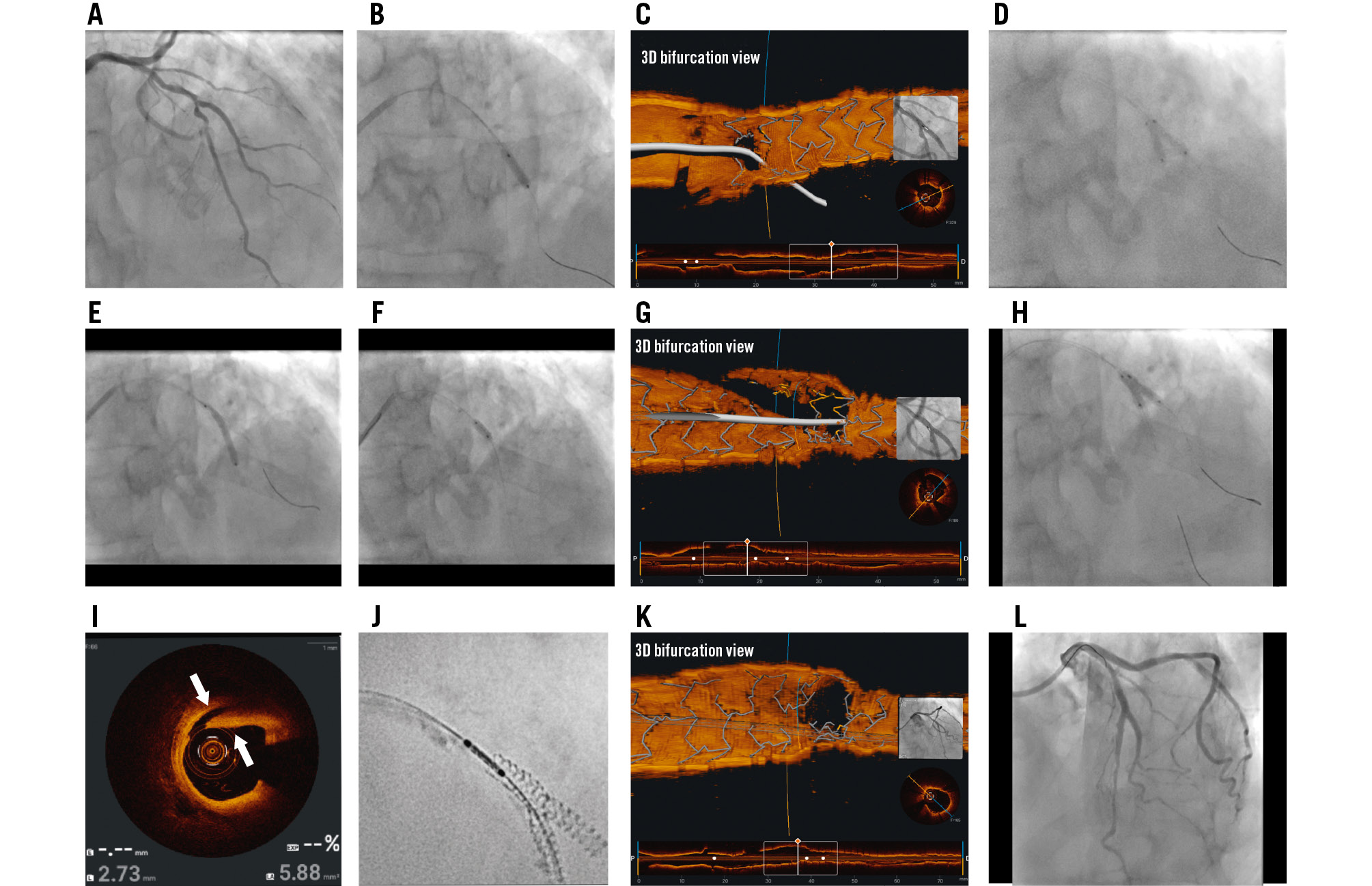
Figure 1. Step-by-step double-kissing single-string culotte assisted by 3D-OCT. A) Baseline angiography in cranial view showing severe complex bifurcation LAD/D2 disease (Medina 1,1,1). B) A 2.75×12 mm XIENCE stent deployed in the D2 with minimal protrusion into the LAD. C) 3D-OCT showing the new LAD guidewire through the first strut of the D2 stent. D) First kissing balloon inflation (KBI) with a 3.0×12 mm non-compliant (NC) balloon. E) Deployment of a 2.75×28 mm XIENCE stent in the LAD. F) Proximal optimisation technique using a 3.5×8 mm NC balloon. G) 3D-OCT showing rewiring of the D2 through the distal cell. H) Second KBI with a 3.0×12 mm NC balloon. I) Proximal edge dissection involving the media layer on OCT (white arrows). J) Coverage of the edge dissection with a 3.0×8 mm XIENCE stent as shown by stent enhancement. K) Final 3D-OCT showing a widely patent D2 ostium. L) Final angiogram showing good results of the LAD/D2 stents. Total skin radiation dose: 924 mGy; fluoroscopy time: 26.1 minutes; contrast volume: 170 mL. 3D: three-dimensional; D2: second diagonal; LAD: left anterior descending artery; OCT: optical coherence tomography
Conflict of interest statement
E.B. Wu has received consulting honoraria from Abbott. B. Wong has no conflicts of interest to declare.
