Umihiko Kaneko, Yoshifumi Kashima, Daitaro Kanno, Tsutomu Fujita
AsiaIntervention 2018;4:108-109, DOI: 10.4244/AIJ-D-18-00002
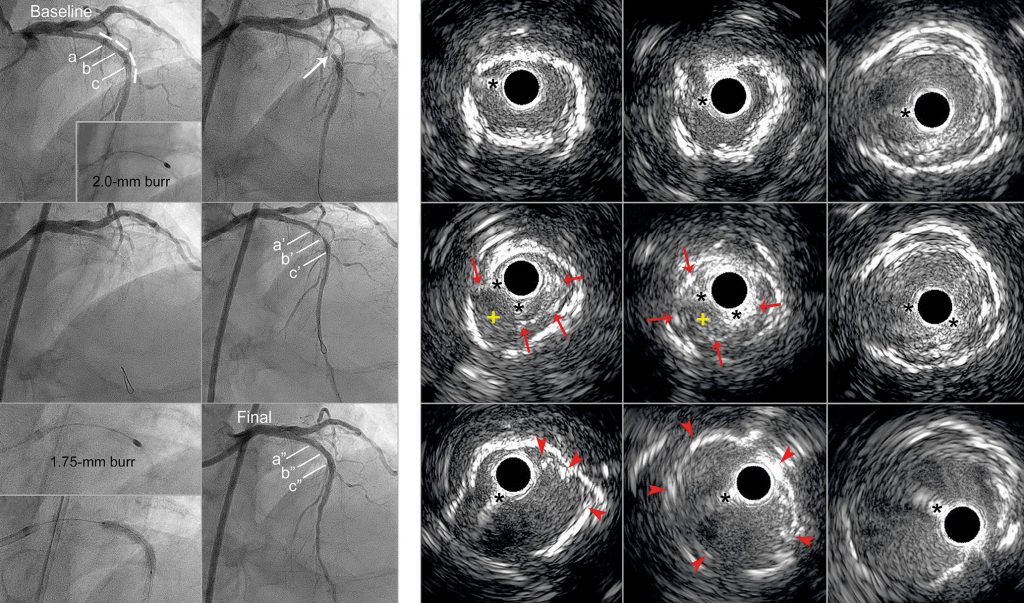
An 83-year-old man was admitted for unstable angina. The angiogram showed in-stent restenosis of a 2.5 mm cobalt-chromium everolimus-eluting stent in the left anterior descending (LAD) artery (fractional flow reserve, 0.73) that had been underexpanded due to heavy calcification five years earlier (Panel A, dotted line, Moving image 1). Baseline intravascular ultrasound (IVUS) revealed the underexpanded stent in the area of continuous calcification with optimal stent apposition (Panel a-Panel c). Rotational atherectomy (RA) of the underexpanded stent was required; however, neither a 2.0 mm (Panel B) nor a 1.75 mm rotablation burr could cross the stent without significant deceleration, leading to subtotal occlusion with ST-segment elevation in the precordial leads (Panel C, arrow). A 2.0 mm balloon catheter or a 1.25 mm burr also could not cross; subsequently, the LAD became totally occluded (Panel D). As a bail-out procedure, a second floppy guidewire was used to pass through the other remaining lumen inside the occluded stent to restore coronary flow (Panel E). IVUS demonstrated that the distorted stent struts had been ablated by the rotablation burr (Panel a’-Panel c’: red arrows, yellow asterisks indicate the deformed stent that remained in a circle; Moving image 2). Following guidewire exchange for the ROTAWire™ Extra Support (Boston Scientific, Marlborough, MA, USA) with the aid of a microcatheter, we managed to ablate the deformed, undilatable stent using a 1.75 mm burr at 210,000 rpm with deceleration (7,000 rpm) (Panel F). Angioplasty with a 3.5 mm scoring balloon and 3.5 mm drug-coated balloon re-established good coronary flow with excellent stent expansion (Panel G, Panel H, Panel a”-Panel c”: red arrowheads; Moving image 3). No restenosis had occurred at the one-year follow-up. This is the first report of acute coronary occlusion due to stent deformation caused by RA of an underexpanded stent. Use of a relatively large burr (burr artery ratio, 0.75) deformed and crushed the underexpanded stent, which caused thrombus formation and the accumulation of tissue fragments that led to acute coronary occlusion. RA of the deformed, undilatable stent was successful using the second guidewire in the remaining lumen, resulting in excellent stent expansion. For RA of the underexpanded stent in this case, a step-up procedure starting with a 1.5 mm burr (i.e., burr-to-artery ratio of 0.6) up to a 1.75 mm burr might have been a safer approach.
[/custom_font]
Moving image 1. Baseline intravascular ultrasound showing residual stent underexpansion with heavy and circumferential calcification.
Moving image 2. Intravascular ultrasound after the second guidewire crossing, demonstrating the distorted stent struts, suggestive of stent deformation caused by RA.
Moving image 3. Final intravascular ultrasound examination showing excellent stent expansion with correction of the deformed strut.
To download the full article, please click below.