Percutaneous double-balloon valvotomy for tricuspid stenosis is a promising technique, particularly in patients with prohibitive surgical risk. We report two cases of percutaneous valvotomy in rheumatic tricuspid stenosis.
Two females in their forties with rheumatic heart disease presented with severe symptomatic tricuspid stenosis, severe fixed orifice tricuspid regurgitation (TR), and good biventricular function. The first patient had a previous mitral valve replacement (TTK Chitra Heart Valve 25 mm [TTK Healthcare]) with normal prosthetic valve function. The second patient had concomitant severe mitral stenosis. The tricuspid annuli measured 36 mm and 30 mm, respectively. Both patients had an intermediate risk of surgery as per the Society of Thoracic Surgeons score. The pros and cons of surgery were discussed, and, in view of both patients’ reluctance to undergo tricuspid valve surgery and affordability issues, it was decided to perform a transcatheter intervention.
Both right and left femoral venous access were obtained. Two balloons (Accura Balloon Catheter PTMC Balloon [Vascular Concepts]) were introduced via the femoral veins across the tricuspid valve into the right ventricle. Due care was taken to ensure the positioning of the balloons across the tricuspid orifice. This was ensured by inflating and withdrawing the larger balloon first until some resistance was felt. The indentation at the waist marked the plane of the annulus. Once the first balloon was hinged at the annulus, the second balloon was inflated and retracted to the level of the annulus. Once both balloons were positioned at the annulus, they were simultaneously inflated until the waists disappeared (Figure 1A). This required excellent coordination between the two operators (Moving image 1). The haemodynamic parameters and details of the preprocedure and post-procedure echocardiography are summarised in Supplementary Table 1. The pre- and post-procedure haemodynamic tracings from the first patient are shown in Figure 1B and Figure 1C, respectively. No worsening of TR was noted. In the second patient, intraoperative transoesophageal echocardiographic images of the native tricuspid valve and the inflated balloons across the tricuspid annulus were obtained, as shown in Figure 1D–Figure 1E–Figure 1F. At 1-year follow-up, no restenosis was noted, but there was severe TR. However, both patients were asymptomatic at 1 year post-procedure. These findings are summarised in Supplementary Table 2.
The effective balloon diameter (EBD) was estimated using standard charts and calculated using the formula: EBD=0.82(D1+D2), where D1 and D2 were the balloon diameters1. A 28 mm balloon and a 22 mm balloon with an EBD of 40 mm and two 22 mm balloons with an EBD of 36 mm were used in the first and second patient, respectively. The unique profile of the Accura balloon ensures that the distal portion of the balloon inflates first and passes freely to the apex of the ventricle, like a balloon-floatation tip. The balloon is then withdrawn until some resistance is felt at the level of the commissures. Finally, full inflation expands the proximal portion of the balloon, which is followed by the disappearance of the central waist2. This mechanism has been adopted for tricuspid valvotomies. However, this adoption represents certain intrinsic technical difficulties due to differences in the anatomy of the mitral and tricuspid valves and the right-sided and left-sided chambers of the heart3.
The tricuspid valve is the largest heart valve with an area of 7-9 cm2. The annulus may be further dilated in the presence of severe tricuspid regurgitation. Therefore, we adopted upfront use of the double-balloon technique for these large annuli, as single-balloon dilation is often ineffective.
The shape of the Accura balloon ensures stability and prevents slippage during inflation. Easier trackability, lower cost, and the ability to deliver higher and more stable pressures represent its advantages over the Inoue balloon (Toray Industries)4. The right atrium is hugely dilated in severe tricuspid stenosis, which poses great difficulty in crossing the stenotic valve. However, concomitant presence of severe tricuspid regurgitation helped in our case for facilitating the passage of the balloons across the tricuspid annulus. Another important consideration is that the leaflets and the chordae of the tricuspid valve are thinner, and, thus, risk of chordal rupture may be higher in tricuspid valvotomy5. Therefore, double-balloon tricuspid valvotomy may be considered in patients with isolated tricuspid valve disease with predominant stenosis and fixed orifice TR in resource-restricted settings.
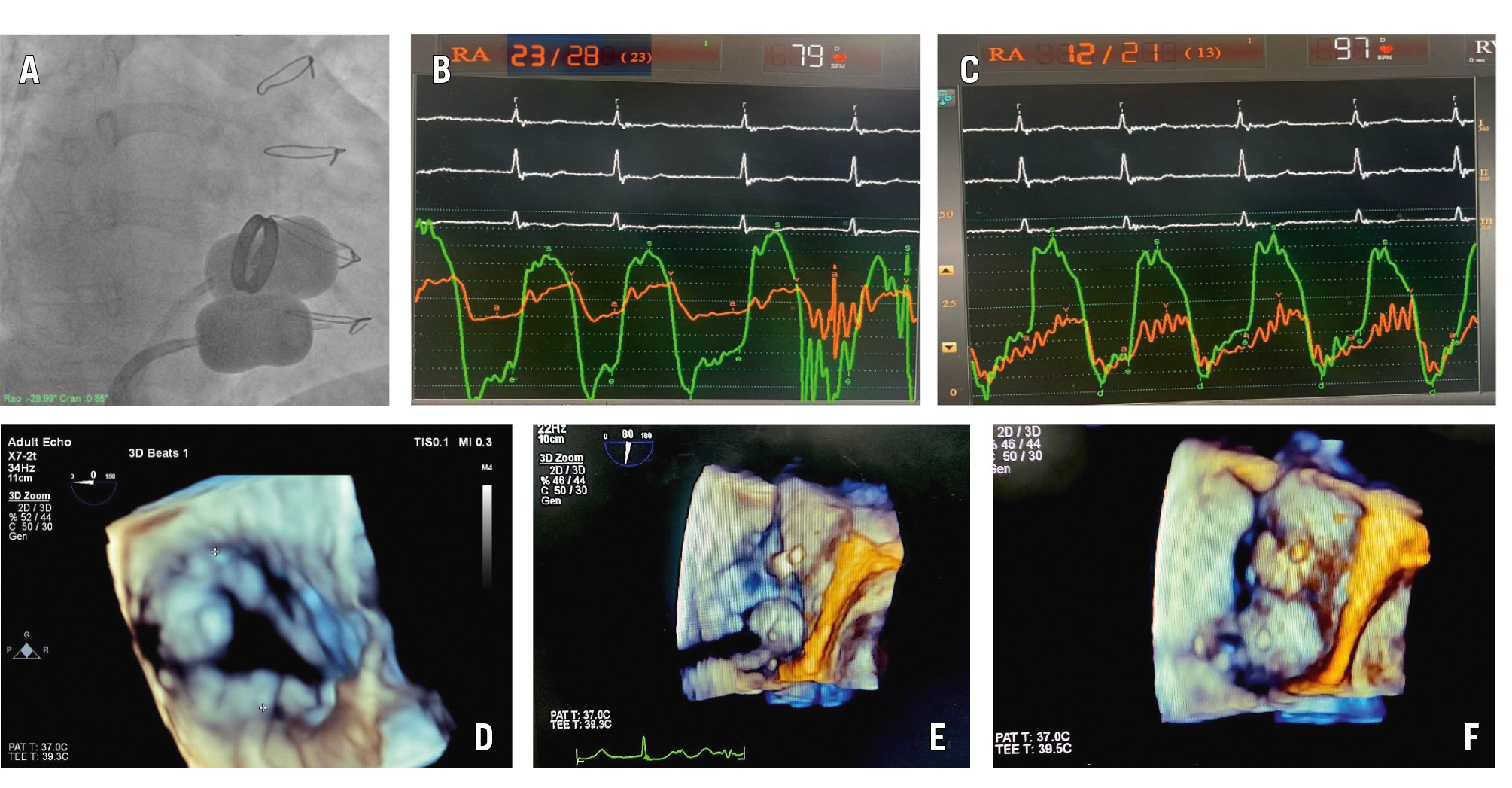
Figure 1. Fluoroscopic image, haemodynamic tracings, and 3D transesophageal echocardiographic images of double-balloon tricuspid valvotomy. A-C) First patient: (A) fluoroscopic image of 2 inflated Accura balloons across the tricuspid valve; (B) preprocedure haemodynamic tracing with TVG of 18 mmHg and (C) post-procedure tracings showing no gradient. (D-F) Second patient’s 3D transoesophageal echocardiographic images: (D) native tricuspid valve; (E, F) partially and fully inflated Accura balloons across the tricuspid valve. 3D: three-dimensional; TVG: tricuspid valve gradient
Conflict of interest statement
The authors have no conflicts of interest to declare.
