In-stent restenosis (ISR) continues to remain one of the major complications with intracoronary stents. The incidence of ISR with current-generation drug-eluting stents is around 4.4% at 5 years1. Identifying the mechanism of ISR holds the key to its successful management2.
A 65-year-old diabetic male, with a previous history of percutaneous coronary intervention (PCI), presented with acute coronary syndrome. His coronary angiogram revealed in-stent restenosis of the ostioproximal left anterior descending artery (LAD) (Figure 1A). During LAD PCI, the predilation balloon encountered resistance during tracking through the left main coronary artery (LMCA). Enhanced cineangiography imaging showed deformed stent struts protruding into the LMCA lumen (Figure 1B). Intravascular ultrasound (IVUS) revealed the abluminal passage of the LAD wire (Figure 1C, Figure 1D). Rewiring of the LAD, followed by high-pressure balloon dilation in the LMCA, led to removal of the deformed stent struts, with luminal wire positions being confirmed on IVUS (Figure 1E–Figure 1F–Figure 1G). The LAD ISR was further treated using a drug-coated balloon followed by kissing balloon inflation in the distal LMCA (Figure 1H, Figure 1I). Fully apposed LMCA stent struts were visualised on enhanced cine images along with excellent minimal stent areas achieved on IVUS (Figure 1J–Figure 1K–Figure 1L).
In our case, inadvertent manipulation of the guide catheter, at the end of the previous procedure, likely resulted in stent deformation. This case highlights the indispensable role of intravascular imaging in identifying the exact mechanism of ISR, as strut deformation can be easily missed on simple angiography. Mechanical causes of ISR (stent deformation, fracture, underexpansion) need to be identified and appropriately corrected to achieve optimal outcomes. Routine use of enhanced cineangiography in clinical practice should be encouraged as it helps to quickly identify stent fractures and deformation. Wiring of vessels with deformed stent struts should be carried out cautiously, and the final wire position should always be confirmed using intravascular imaging. This case highlights a rare, yet important, mechanical cause of ISR, reinforcing the critical role of intravascular imaging in identifying and guiding the treatment of such complex scenarios, which may otherwise be missed by angiography alone3.
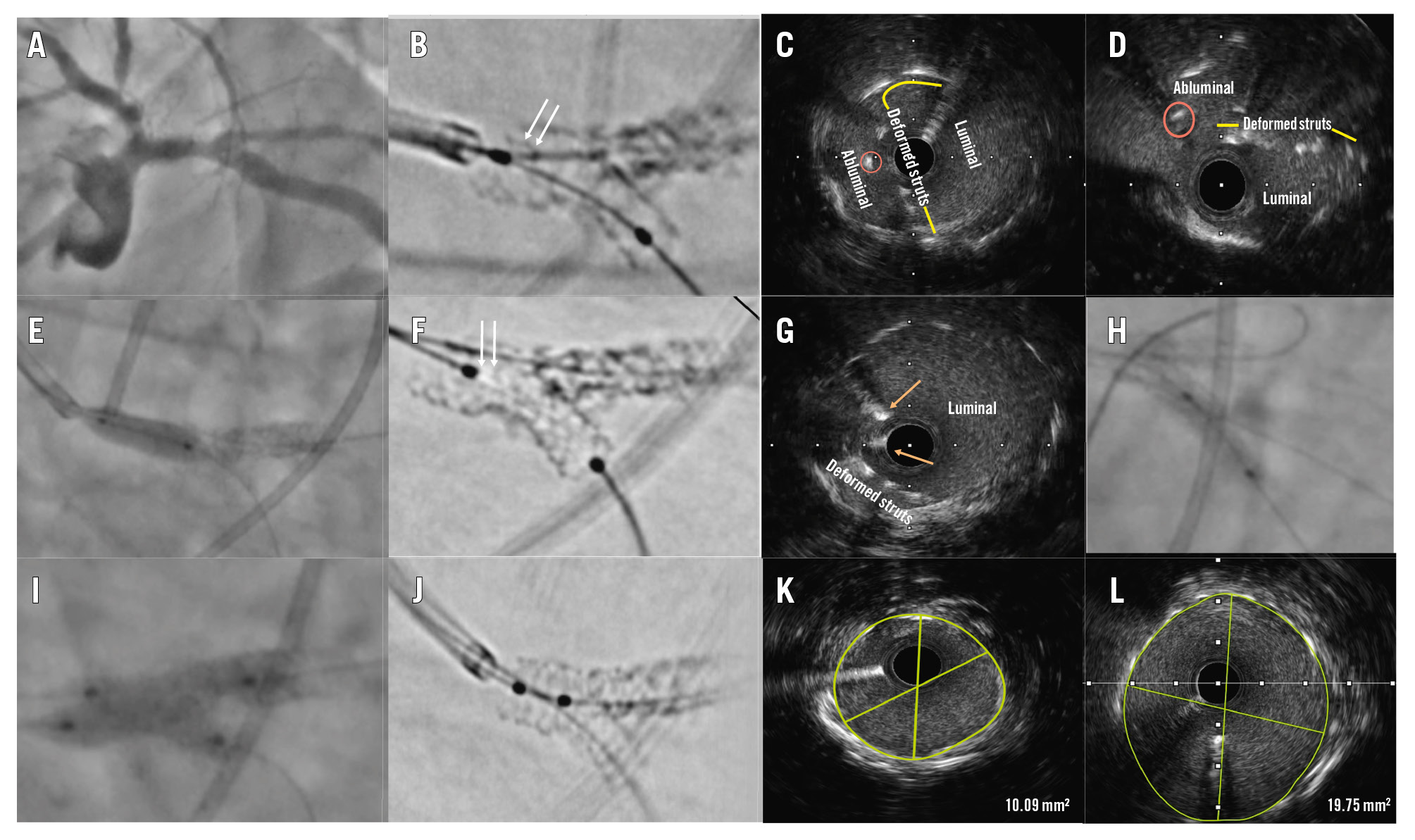
Figure 1. Intraprocedural findings. A coronary angiogram revealed in-stent restenosis of the ostioproximal LAD (A). An enhanced cine image showed deformed stent struts (white arrows) protruding into the LM lumen (B). Intravascular ultrasound showed deformed struts in the vessel lumen (yellow line) along with the LAD wire (orange circle) going behind the deformed struts (abluminal position; C, D). Balloon dilation of the LM stent was performed (E), which led to the apposition of struts (white arrows), seen on an enhanced cine image (F). Repeat IVUS showed displacement of the deformed struts with a luminal position of both wires (orange arrows; G). A drug-coated balloon was used in the LM-LAD (H), followed by kissing balloon inflation at the distal LM bifurcation (I). The stent struts were well apposed on a cine image (J), with MSAs of 10.09 mm2 and 19.75 mm2 in the LAD and LM, respectively (K, L). IVUS: intravascular ultrasound; LAD: left anterior descending artery; LM: left main artery; MSA: minimal stent area
Conflict of interest statement
The authors have no conflicts of interest to declare.
