Author: Fumiaki Nakao
A 77-year-old woman, who had previously had single crossover stenting and kissing balloon dilation (KBD) for a bifurcation lesion of the left anterior descending artery (LAD) and the diagonal branch (Dg), had percutaneous coronary intervention performed for restenosis of the Dg with angina (Figure 1A). Guidewires were inserted to the Dg and the LAD. After the Dg was predilated, a platinum-chromium everolimus-eluting stent (PROMUS Element™ 2.5×16 mm; Boston Scientific Co, Marlborough, MA, USA) was deployed from the LAD to the Dg (Figure 1B) with only one strut overlapping as confirmed by intravascular ultrasonography (IVUS). The guidewire was recrossed to the distal LAD through the stent cell with x-ray fluorographic guidance (Figure 1C), confirmed by IVUS. After KBD was performed, final coronary angiography showed a good result (Figure 1D).
Final instant stent-accentuated three-dimensional optical coherence tomography (iSA3D-OCT) reconstructed using an off-line workstation showed that the reverse minimum overlapping culotte stenting (R-MOCS) had been achieved (Figure 1E, Figure 1F).
Side branch (SB) restenosis is one of the issues with a single-stent strategy for a bifurcation lesion. Culotte stenting or T-stenting and small protrusion (TAP) technique has been performed for an SB restenosis if additional stenting was needed. R-MOCS may be an effective strategy for a restenosis of a gently angled SB at points of lesser influence to the main vessel than culotte stenting, and lesser metallic carina than the TAP technique.
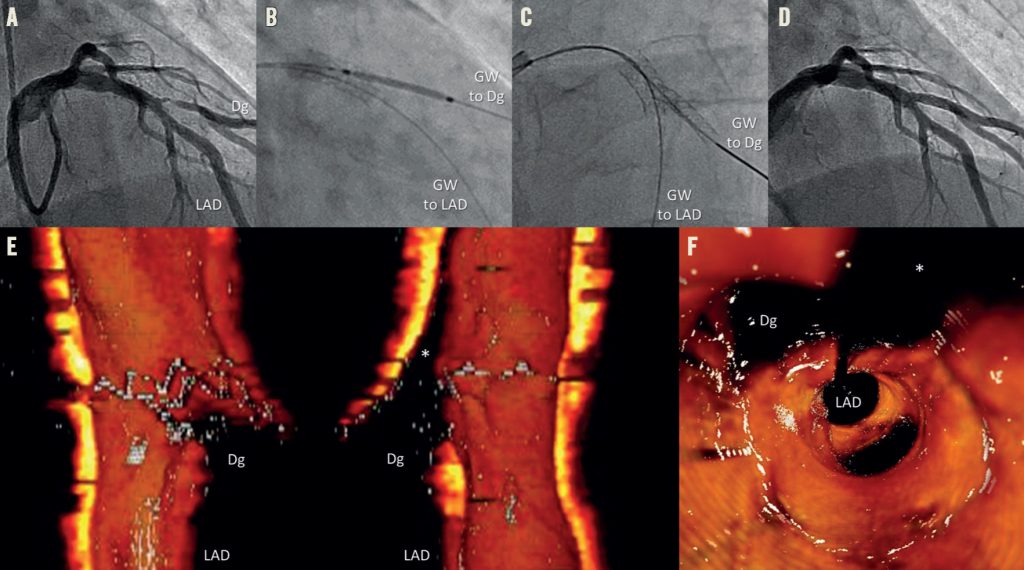
Figure 1. Reverse minimum overlapping culotte stenting (R-MOCS) for side branch restenosis. A) Baseline coronary angiography showing restenosis of the diagonal branch (Dg). B) A platinum-chromium everolimus-eluting stent was deployed from the left anterior descending artery (LAD) to the Dg. C) Guidewire (GW) recrossed to the distal LAD. D) Final angiographic result. Longitudinal cut-away view (E), and fly-though view (F), of final iSA3D-OCT showing R-MOCS. Asteriks indicate GW shadow artefacts.
Supplementary data
[/custom_font]